Do Stroke Characteristics Change During a High-Intensity 12-minutes Corridor Wheelchair Propulsion Test in Experienced Manual Wheelchair Users?
Dany Gagnon, PT, PhD1,2 ; Michael L. Boninger MD1-3 ; Jennifer L. Collinger BS1-3 ; Bradley G. Impink BS1,3 ; Alicia Koontz, RET, PhD1,3 .
1 Human Engineering Research Laboratories, VA Pittsburgh Healthcare System,
7180 Highland Dr., Building 4, 151R-1, Pittsburgh, PA 15206
2 Department of Physical Medicine and Rehabilitation, University of Pittsburgh
3 Department of Bioengineering, University of Pittsburgh
ABSTRACT
A high-intensity wheelchair propulsion test (WPT) was recently developed to trigger acute median nerve and rotator cuff tendon changes. This test mimics many manual wheelchair propulsion skills and perturbations routinely encountered in daily life that may exacerbate secondary upper limb impairments: start-ups, steady-state propulsion, turns and stops. Nineteen participants completed the standardized high-intensity 12-minute corridor WPT on concrete floor along a figure 8 course. Participant’s wheelchair were fitted bilaterally with instrumented wheels (SMARTwheel®) to collect key spatiotemporal and kinetic parameters for the start-up and steady-state strokes during the WPT12min. Effective neuro-motor adaptation processes may have contributed to maintain, even favorably change, stroke characteristics expected to be negatively affected by upper limb fatigue during the WPT12min. Methodological issues also need consideration as they may have under-estimated the magnitude of the stroke characteristic changes documented in this study.
KEY WORDS
Biomechanics, Fatigue, Rehabilitation, Upper Extremity, Wheelchair.
BACKGROUND
The development of fatigue in the upper limb during manual wheelchair propulsion, which results in part from substantial upper limb muscular efforts, may increase an individual's risk of developing secondary upper limb impairments, especially at the shoulder or wrist joint (1). In fact, a high prevalence of shoulder (30-60%) and wrist (40-66%) joint complaints have been reported among long-term manual wheelchair users (MWUs) over the years (1).
In attempts to quantify the potential risk of developing secondary upper limb impairments, the biomechanics of manual wheelchair propulsion during fatigue have been investigated in simulated laboratory environments (2-5). In most of these studies, MWUs were instructed to propel their own wheelchair at a comfortable speed (sub-maximal protocol) on an ergometer during a prolonged period of time. Compensatory changes documented during these tests, such as an increase in resultant force at the pushrim for example, may exacerbate the development of secondary impairments at the upper limb during propulsion. However, cautiousness is advised when inferring from these findings as testing conditions differ substantially from the rigors of routine wheelchair propulsion observed in daily life.
For this reason, a high-intensity 12-minute wheelchair propulsion test (WPT12min) was recently developed. This performance-based test mimics many manual wheelchair propulsion skills and perturbations routinely encountered in daily life: start-ups, steady-state propulsion, turns and stops. This strenuous test was designed to imitate the repetitive conditions often encountered by MWUs which are believed to contribute to the development of secondary upper limb impairments. To elucidate potential causes underlying these biological alterations observed after the WPT12min, a comprehensive assessment of the stroke characteristic changes during its completion is of interest.
RESEARCH QUESTION
The objective of this study was to quantify the effects of a high-intensity corridor WPT12min on key stroke characteristic outcomes for the non-dominant upper limb in experienced MWUs. As the state of fatigue progresses during the WPT12min, it was hypothesized that stroke cadence, total force applied to the pushrim (Fresultant), rate of rise of force (RORForce) and moment out of the plane of the wheel (Mp) increases whereas the distance per stroke, the propulsion velocity, and application of force directly contributing to forward motion (Ftangantial) decreases.
METHOD
Participants:
A convenience sample of 19 long-term MWUs (18 males; 1 female) with various diagnoses (spinal cord injury (n=16); multiple sclerosis (n=2) and above-knee amputation (n=1)) were recruited during the 2007 National Veterans Summer Wheelchair Games hosted in Milwaukee (Wisconsin) to participate in this study. On average (mean±1SD), participants were 50.4 ±8.9 years of age, 1.78±0.07m in height, weighed 85.5±16.8kg, and had been using a manual wheelchair as their primary mode of mobility for the past 12.9±10.6 years. At the time of testing, no participant complained of musculoskeletal impairments affecting their trunk and upper limbs, nor any other condition, which could have altered their ability to manually propel their wheelchair. Ethical approval was obtained from the Internal Review Board of the VA Healthcare System Pittsburgh. Participants reviewed and signed an informed consent form before entering the study.
Wheelchair propulsion test:
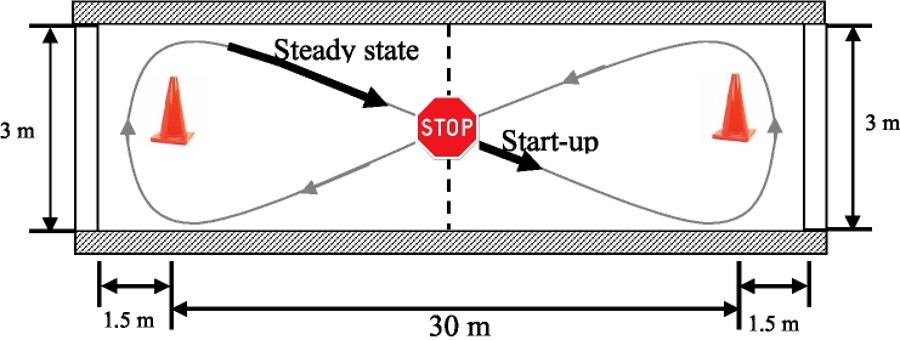 Figure 1. (Click for larger view)
Figure 1. (Click for larger view) All participants completed a standardized high-intensity corridor WPT12min on concrete floor along a figure 8 course (Figure 1). Before starting the test, participants were instructed to propel their wheelchair as fast as possible over the entire course, and to rapidly come to a complete stop upon completion of each loop before pushing around the subsequent loop. During the test, participants continuously propelled their wheelchair for four minutes (first segment), and then rested for 90 seconds. This sequence was repeated two more times (middle and last segments) to obtain a total high-intensity propulsion time of 12-minutes. No familiarization period was conducted prior to data collection as all participants were experienced MWUs.
Kinetic data collection:
During the WPT12min, each participant’s wheelchair was fitted bilaterally with instrumented wheels (SMARTwheel®; Three River Holding, Mesa, Az) to record three-dimensional forces (240 Hz) and moments applied to the pushrims during the first figure 8 completed during each of the three segments of the test. These instrumented wheels, once mounted on a participant’s wheelchair, closely imitate the usual wheels’ size, position and orientation.
Stroke characteristic outcomes:
Key spatio-temporal and kinetic parameters for the start-up (first three strokes) and steady-state portions (all strokes completed) of each segment of the WPT12min were computed during the push phase of each completed cycle (recovery phase not included) using a customized Matlab program (The Mathworks, Natick, MA). Spatio-temporal outcomes include stroke cadence, push and recovery times, distance traveled per stroke as well as the mean and peak propulsion velocities. Kinetic outcomes included the total force applied to the pushrim (Fresultant), the force directly contributing to forward motion (Ftangantial), the force directed inward toward the axle of the wheel (Fradial), the rate of rise of force (RORForce) and the moment out of the plane of the wheel (Mp).
Statistics:
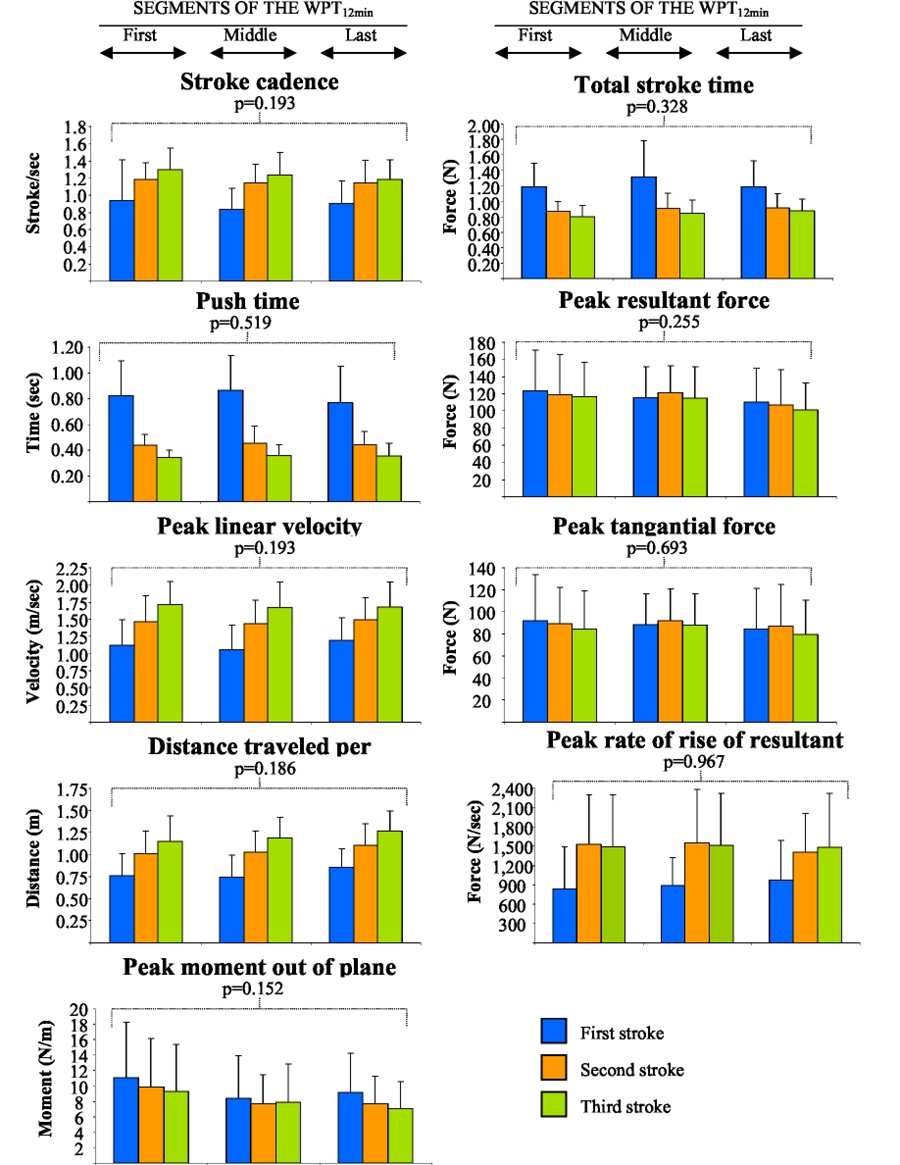 Figure 2. (Click for larger view)
Figure 2. (Click for larger view) For all start-up outcomes, repeated measures analyses of variance (ANOVA) [3 strokes (first, second and third) X 3 test’s segments (first, middle and last)] were applied to determine if stroke characteristics changed during the test. For the steady state outcomes, one-way repeated measures ANOVA were used to explore how stroke characteristics differed across the three segments of the test (first, middle and last). A level of significance of 0.05 was selected for all tests. Statistical analyses were performed using SPSS® software Windows (version 14.0).
RESULTS
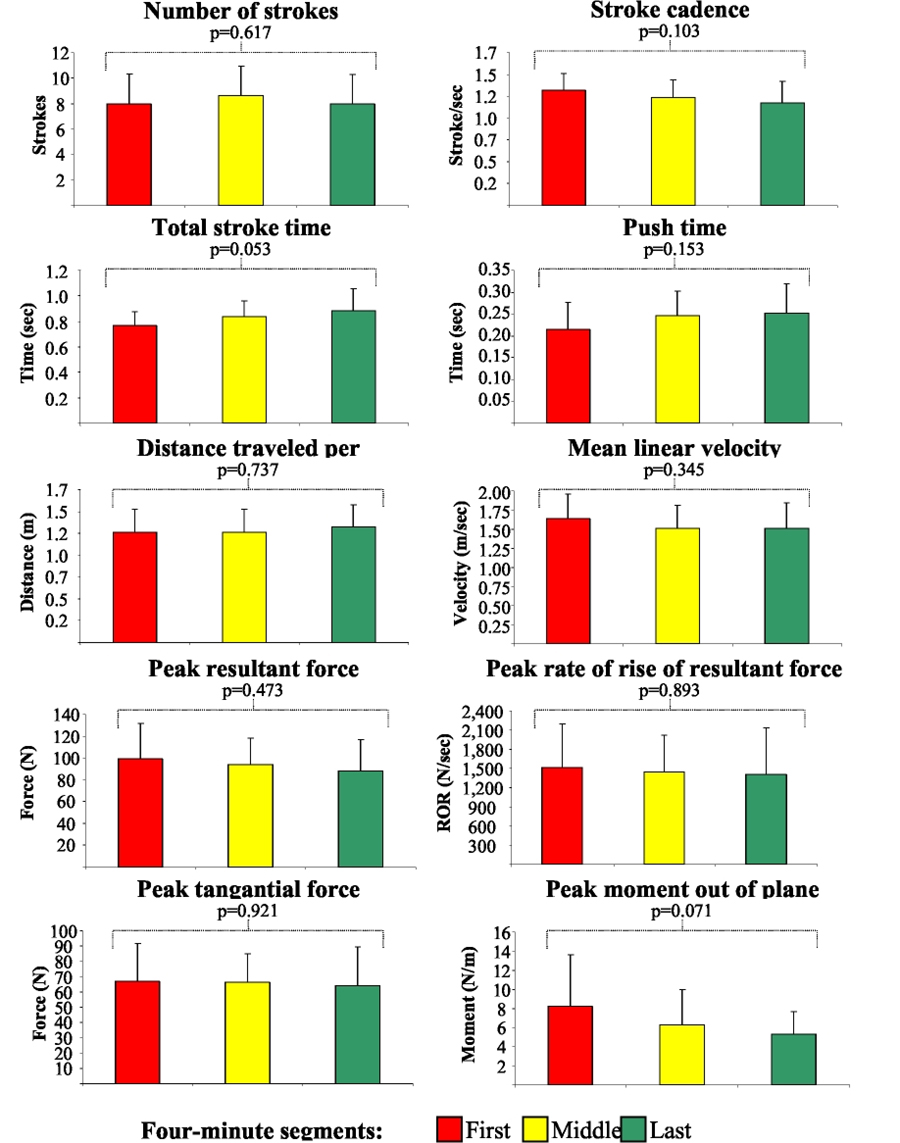 Figure 3. (Click for larger view)
Figure 3. (Click for larger view) All participants were able to complete the high-intensity corridor WPT12min at their self-selected maximum velocity. For both the start-up (Figure 2) and steady state strokes (Figure 3), no significant difference was found across the three distinct segments for the stroke characteristic outcomes of interest. Few differences were found across the start-up strokes (Figure 2).
Unexpectedly, some of the changes in stroke characteristics observed, though not statistically significant, remain clinically relevant as they may indicate that a more effective propulsion technique may favorably evolve over time during this propulsion test. For example, a tendency for the stroke frequency, peak resultant force and peak moment out of plane to decrease while maintaining linear velocity certainly need consideration.
DISCUSSION
The completion of the high-intensity corridor WPT12min placed a high mechanical demand on the upper limb, as evidenced by the results of the start-up (5) and steady state (6) segments in comparison to reference values documented for self-selected or sub-maximal overground wheelchair propulsion. This mechanical load imposed on the upper limb structures, triggered by the high-intensity testing protocol, needs to be counteracted by the generation of explosive upper limb moments to move and stabilize trunk and upper limb segments and joints, respectively. Consequently, it was hypothesized that upper limb muscular fatigue would develop over time and would lead to stoke characteristic changes. The results of this study do not support this hypothesis.
As the number of completed figure 8 laps increases during the test, the development (early motor stage) and refinement (motor consolidation) of a rapid and coordinated motor performance (internal model) is expected. The accrued reliance on such an internal model allow the central nervous system to adequately pre-plan muscle activity required to perform the tasks incorporated into the test (reduced muscular efforts), even before motion-dependant feedback becomes available, which may have prevented the rapid depletion of the muscular strength reserve. It should also be noted that the test solicits multi-joint upper limb movements that can be realized by an almost unlimited number of bi- and mono-articular muscle recruitment strategies (muscular redundancy), meaning that a large inventory of effective compensatory strategies may have been used during the test. These two neuro-motor adaptation mechanisms may have masked the early effects of localized upper limb fatigue verbally expressed after the current test by all participants. Moreover, they most likely explain why stroke characteristics remained unchanged, or even tended to favorably evolve, during the test.
Finally, a special attention needs to be given to the fact that only the first figure 8 lap, completed immediately after a 90-second rest period, was recorded in the current study. This may have prevented the detection of fatigue-related stroke characteristic changes occurring later during each segment. Ideally, recording of the total duration of the test is suggested to thoroughly assess the effect of fatigue over time. Minimally, the first and last completed figure 8 laps should be recorded to document overall stroke characteristic changes during the WPT12min. Grading the rate of perceived exertion, even of some key cardio-respiratory parameters, may also be of interest in an effort to refine this test in the future. Consideration to reduce the 90-second rest periods’ duration, initially planned to avoid over-exertion, may also be indicated especially if testing wheelchair athletes.
CONCLUSION
The newly-developed high-intensity corridor WPT12min represents an alternative to traditional wheelchair ergometer tests. This test was found to be useful, safe and easy to administer. Moreover, it is incorporating many manual wheelchair propulsion skills and perturbations encountered in daily life: start-ups, steady-state propulsion, turns and stops. Effective neuro-motor adaptation processes may have contributed to maintain, even favorably change, key stroke characteristics expected to be negatively affected by upper limb fatigue during the WPT12min. Methodological issues also need consideration as they may have under-estimated the magnitude of the stroke characteristic changes documented in this study. In the future, the continuous recording of the stroke characteristics need to be considered if computing outcome measures in clinical practice or research situations.
REFERENCES
- Consortium for Spinal Cord Medicine Clinical Practice Guidelines. (2005) Preservation of upper limb function following spinal cord injury: a clinical practice guideline for health-care professionals. First ed. Washington (DC): Paralyzed Veteran of America.
- Rogers MM et al.(1994) Biomechanics of wheelchair propulsion during fatigue. Arch Phys Med Rehabil; 75:p85-93.
- Rogers MM et al. (2003) Upper-limb fatigue-related joint power shifts in experienced wheelchair users and nonwheelchair users. J Rehabil Res Dev; 40(1):p.27-37.
- Bernasconi SM et al. (2007) Changes in oxygen uptake, shoulder muscles activity, and propulsion cycle timing during strenuous wheelchair exercise. Spinal Cord; 45(7):p.468-474.
- Koontz AM et al. (2005) A kinematic analysis of manual wheelchair propulsion during start-up on selected indoor and outdoor surfaces. J Rehabil Res Dev; 42(4):p.447-458.
- Koontz AM et al. (2008) Manual wheelchair propulsion patterns on natural surfaces. ARCH Phys Med Rehabil [In Press].
ACKNOWLEDGEMENTS
This study was supported by the Department of Education, National Institute on Disability and Rehabilitation Research as the first sponsor and the National Institutes of Health. Dany Gagnon holds a post-doctoral scholarship from the Fond de la recherche en sant6 du Qu6bec (FRSQ).
Author Contact Information:
Dany Gagnon, Human Engineering Research Laboratory, VA Pittsburgh Healthcare System, 7180 Highland Dr., Building 4, 151R-1, Pittsburgh, PA 15206; Phone: (412)365-4850; Fax: (412) 365-4858; email: gagnond@herlpitt.org